misfit migrants
Crackerjacks. Cohorts. Greenhorns. Frenemies.
Guest contributors run the gamut, but they all pretty much rock.
Guest contributors run the gamut, but they all pretty much rock.
|
“I didn't hear a word she said. I was looking at the James Brown wig.”
FOX’s Bill O’Reilly made a statement that was thoughtless and mean-spirited about Congresswoman Maxine Waters (Note: He has since apologized). Make no mistake about that. While I don’t take the full knee-jerking position, I will say he didn’t need to hit Congresswoman Waters with an insult about her hair when there is enough to address about her that has nothing to do with her physical appearance. There isn’t much I agree with O’Reilly on, but I do think that Congresswoman Waters should have her own sitcom. She’s made many outlandish, moronic statements over the years that are more fit for a parody of elected officials than the rhetoric of one who is serious about representing constituents. I’ll even go as far as to say that I don’t think his comments were racist, despite many opinion and news outlets manufacturing it by mentioning Congresswoman Waters is African-American. The fact is that O’Reilly and his ilk in infotainment news have made a career out of potshots and negativity. Whether it’s Keith Olbermann, Bill Maher, O’Reilly, or Sean Hannity, why do we consistently hold our hands over our mouths and feign surprise when they go for low blows? On the other hand, Congresswoman Waters isn’t intimidated or frightened of O’Reilly, conservative media, or anyone else. The real insult is that she has made an entire career out of feeding spite to her “enemies” and helping herself to taxpayer money rather than fighting for the constituents she represents. These folks are still hurting due to last decade's recession, crime at the hands of gangs (due to police departments and officers fearing racial discrimination suits and sanctuary governments protecting known criminals), and efforts to push many of her electorate into a neighboring county due to economic collapse and gentrification. While she doesn’t deserve to be attacked because of her looks, let’s not act as if she needs the kid glove treatment. Calling her fellow legislators “demons,” telling a large group of concerned Americans that she intends to help them go “straight to hell” while she orates more empty promises and divisive rhetoric doesn’t make Congresswoman Waters a very sympathetic character. And if she isn’t “afraid of anybody,” why are people so quick to go to bat for her? She can clearly fight her own battles. Speaking of James Brown wigs, many of the usual suspects aghast at O’Reilly’s cheap shots were roasting FOX Sports’ Pam Oliver and her personal appearance for some NFL Playoff games a few years back. Her wigs were disheveled, looked cheap, and the director either cut to Erin Andrews or showed shots of the crowd and the benches while Oliver was speaking. Those usual suspects were laughing, retweeting memes, and applauding the takedown of a woman who probably just had a few bad days and certainly didn’t deserve such malignant criticism. We only insult or criticize others’ personal appearances when we’ve run out of gas and have nothing more clever to say. We only complain about someone going too far in personal attacks when we support them for personal agendas, political capital, and/or we see part of ourselves in the person that was attacked. Personal attacks should always be condemned, no matter who said them or who was targeted. But try telling that to anyone in any corner of this hyper-partisan climate, and you’re likely to be shot down as a bigot or a knee-jerker. The hypocrisy. Being mean-spirited is not something that social media or the current political climate created. Most of us have it ingrained in us; it’s part of our competitive nature as human beings. The insatiable need to criticize others is something that we can curb, but cannot outright cure. I’ve said many things before that were mean-spirited (be it provoked, out of jealousy, or humor at someone else’s expense). I'll likely slip up, intentional or not. And many things I say I deeply regret in retrospect. But the way we can do better is not to not police what others say; it’s to change what we say and what we do to set the tone. In doing so, we clear our own conscience of negativity.
0 Comments
Guest Contributor Chelie
I just “celebrated” living with Type 1 diabetes for 50 years, and I’d like to share a bit of it with you.
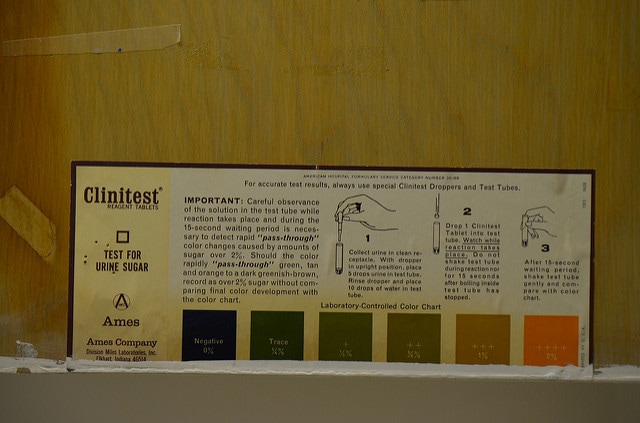
See this little testing kit? 
I carried it around everywhere, once I was diagnosed in 1967 when I was in the first grade. Here’s how it worked: I would take the cover of the kit, turn it upside down, and pee in that part. I’d then (after setting it on the floor and finishing my business) take both parts to the sink. I’d carefully count out 10 drops of urine with the eyedropper into the test tube, add 5 of water, drop in a Clinitest reagent tablet (It’s poisonous! Don’t touch it!), and watch the mixture bubble and foam for exactly 15 seconds. There was a color chart that came with the tablets and I’d compare the color of the solution in the test tube to the chart to know what my sugar level was. If it was blue, it was good. If it was orange, it was bad. (Aside: maybe this is why I don’t like the color orange?) This old testing was so imprecise! Can you imagine, I was injecting a potentially lethal drug (insulin) based on “good” or “bad”!
I had to do this a lot, so I became a good little lab assistant at the tender age of 6. I learned to clean the kit and components in school and home sinks, in church sinks and friends’ sinks. At first it was fun to play scientist, but after a while I hated that little kit. I couldn’t go anywhere without it or my syringes and insulin vials. I inadvertently scared playmates when they saw the needle on the syringe, and probably when I would go into low blood sugar episodes.
(Side Note: I was shocked and embarrassed when I saw “Steel Magnolias” in the theater, being completely blindsided by Shelby’s insulin low. I cried the entire way home. Do I really look and act like that??)
I couldn’t eat anything or drink anything without testing and taking a shot first. I still can’t, but after 50 years I’ve gotten as used to it as I can. Nowadays the testing is a prick of the finger instead of urine, water, and a tablet in a test tube. I’m much happier about that! It’s still not ideal, though. Today’s glucometers, which use a drop of blood on a test strip and are MUCH more accurate, are still not that portable. Here’s mine:
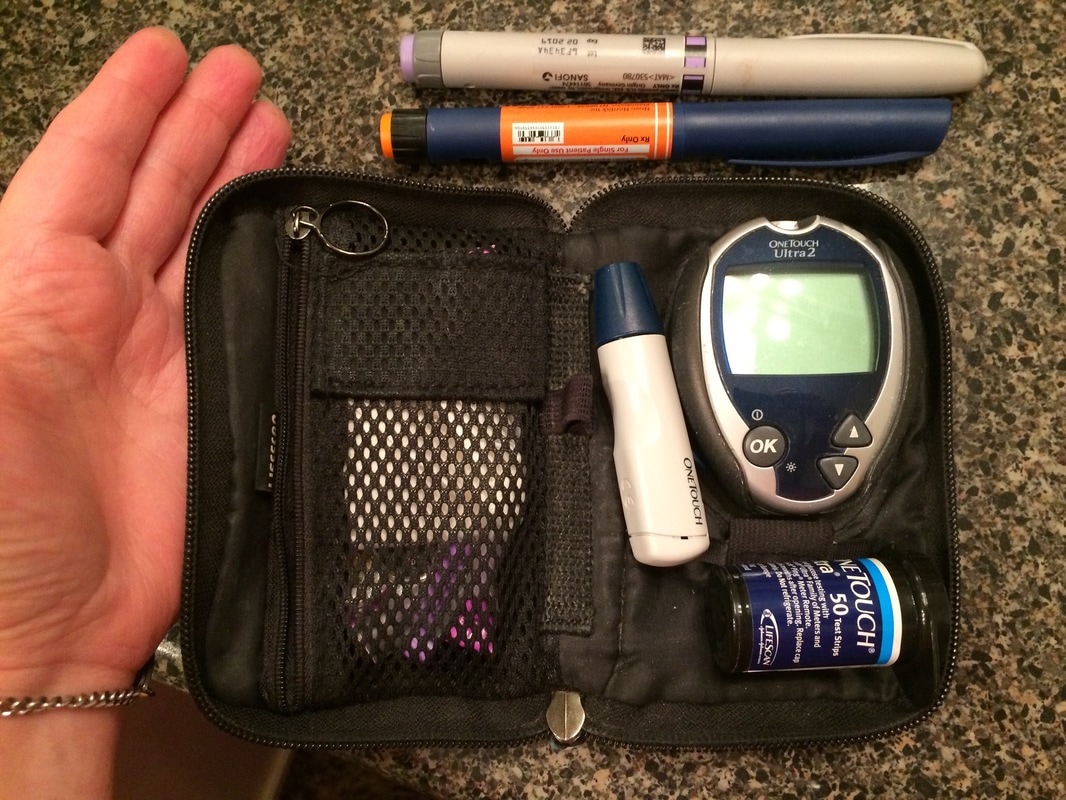
I test a lot, maybe 6 times a day; morning, before every meal, before I get in the car to drive, and at night. That doesn’t count the times I test if I’m feeling low or high. This glucometer and my supplies don’t fit into those tiny purses. The 2 pen-looking things are my insulin; the grey one is my long-acting kind that lasts about 12 hours (I take some of that in the morning and again before bed), and the blue is the short-acting insulin that I take at meals to cover what I’ll eat. I also use it to counteract any high blood sugar. There’s lots of math involved in being a Type 1 diabetic. We count carbs and calculate our insulin dosage that way. Of course, if you get the math wrong, or eat more (or less) than you thought you would, or even if the ingredients of a dish are different than what you anticipated, it causes problems. Timing is a big deal, too. Once I take my insulin, I have to eat within 15 minutes or I run a real risk of having a low. When I’m out, I wince internally as I excuse myself from a table full of people to go to the nearest empty room or restroom and take my insulin, thinking I’m drawing attention to myself or interrupting the flow of conversation. I then try to sneak back to the table and hope the food will be served fast enough.
All this extra stuff I get to carry around and use in order to not die is expensive. My estimate, using actual costs of bare minimum supplies (insulin, needles, and test strips) is $1,600.00 a month. Never mind the quarterly checkups with my endocrinologist, the lab tests she runs to make sure my glucose levels are staying in a reasonable range, or the annual ophthalmologist appointment with dilation and scans to watch my retinas for possible blindness. Type 1 diabetes is constant; you never really forget about it because you can’t. Your blood glucose is subject to not only when and what you eat or don’t eat, but also to activity levels, to hormone levels (what “fun” it is to be a female Type 1!), to stress levels, to sleep levels, to emotions, to EVERYTHING. In spite of how careful I am, and how absolutely God has blessed and watched over me, I still am unable to get my glucose levels where they supposed to be on a daily basis. It just is not possible, and being slightly perfectionistic makes it very, very frustrating. I can’t do what I must do to prevent all sorts of complications. Often I have to eat when I don’t want to (low blood sugar makes me queasy, or it’s lunch time whether I’m hungry or not) or I can’t eat when I really want that steak at 9 pm. You see, the problem with artificial insulin is that if you use it too much, you develop an intolerance for it. So just taking more insulin to eat that donut or drink that milkshake is not a good idea. I must use it sparingly so when I really need it, it will work. It’s a world of dichotomies; the act of eating which keeps me alive is the thing that is killing me. My disease isn’t apparent and it encompasses much of my life. It’s a world where I am required to predict the unpredictable in order to stay alive. Emphasis on TO STAY ALIVE. Closing thought: go and do an image search of “Type 1 Memes”. They’re funny because they’re true, and they may give you a little insight into what it’s like. We T1s tend to have a gallows kind of humor about it.
Regular Contributor Raymond (@RaymondWPS)
President Trump’s ACA Repeal is stirring up emotions on many sides. Some of those strong emotions are coming from the PrEP (Pre-Exposure Prophylaxis for HIV/AIDS) population. @VernumVulero1 beautifully covered a lot of ground with her take on ACA and AHCA, and I tend to agree with most of it. As someone who utilizes Truvada as PrEP and may be affected by ACA repeal and replacement, I’m addressing the fear mongering and how it directly relates to me.
Many co-pay assistance programs are in danger of having funding cut because of Trump’s ACA Repeal. Co-pay assistance programs that many (including myself) utilize thanks to drug manufacturer Gilead and other non-profit organizations that make access to PrEP and other drugs less expensive. But we have all read the fine print and understand that these co-pay assistance programs were never meant to last and could be taken at any day at any time by the drug manufacturer, whether federal funding existed or not. If and when these events happen, we should not be surprised. We should have a backup plan ready to go. Since day one, I've always filled my prescription as soon as I am allowed so that, in the untimely event that the co-pay assistance or coverage under my provider no longer exists, I can come up with a contingency plan to continue or discuss antiquated prevention methods and my health post-PrEP with my doctor. Another concern is how Truvada will be unavailable to those who have an insurance program through the marketplace. I can’t speak for what will happen, but what I do know from a few friends is that many marketplace plans either will not cover any portion of the drug or will only cover portions of the drug if someone is in a serodiscordant relationship (where one has HIV, and the other does not). As for insurance plans through one’s workplace, many people with different illnesses and treatments share the same concerns under the repeal of ACA. I’m not willfully ignorant: I’m aware at any moment coverage of Truvada under my healthcare plan may end. But unlike many, I always had those concerns because nothing is a complete guarantee. It wasn’t under President Obama (“If you like your plan, you can keep your plan.”) and it won’t be under President Trump. Far beyond pillow talk and the ordering of pizza, this is the post-coital reality we need to accept: PrEP allows us the freedom to take control of our sexual health and allows us not to be completely reliant on the word of someone else or their application (or lack thereof) of a condom. But it should also give us the freedom to manage the acquisition of the drug and payment of the drug by any means necessary. We should never believe that any one government program, government organization, or nonprofit has our best interests completely at heart. Have we yet to learn anything from AIDS Healthcare Foundations, their use of nonprofit funds for real estate, their “War on PrEP,” and their avid slut-shaming of the MSM population for sport? Our efforts as users of PrEP should be to mobilize and build nonprofits that will exclusively subsidize these drugs (and drugs for those who are living with HIV) for years to come, with little to no assistance from the government. Our efforts as individuals should be to find health insurance companies and/or work for employers who care enough about our health and our contributions to the workplace that will cover as much of it as possible. Our efforts should be to legally obtain these drugs by other reputable means (whether it is crossing state lines or even traveling out of the country to obtain them). Our efforts should never be to move backward and believe that President Trump will take advancements of HIV/AIDS back to 1981. Our use of Truvada as PrEP has always been an amazing privilege. It has never been a “right” given to us by the government, nor should it be. I don’t want a government that dictates what my prophylaxis measures should be, what partners I choose to entertain in my bedroom, nor what kind of sex I should have. I also don’t want a government (be it under Obama or Trump) that feels the need to deem what is most important for my health and my existence. I don’t want the government (or any other entity) to have that kind of power over me or my sexual freedom. |
 RSS Feed
RSS Feed